
Raoultella ornithinolytica, an encapsulated Gram-negative bacterium, is a member of the Enterobacteriaceae family. It rarely causes invasive infections.1,2 There are underlying conditions such as pathology of biliary system and malignancy in most cases. Although the majority can recover with adequate antibiotic therapy, some cases have a fatal outcome.2–4 A patient from our country with diabetic foot with ensuing bacteremia had been reported.5 That case was successfully treated by tigecycline.
A 37-year old male patient with relapsing acute lymphocytic leukemia (ALL) was admitted to the hematology department for chemotherapy. He had been diagnosed 1.5 year before and had a history of bone marrow transplantation in the previous year. At first day of FLAG (Fludarabine 30mg/m2, cytosine arabinoside (Ara-C) 2g/m2, granulocyte colony stimulating factor (G-CSF) 5μg/kg/day) chemotherapy, febrile neutropenia developed and piperacillin–tazobactam 4.5g intravenously (iv) every 6h was started. Fever was under control in third day, but recurred after 12 days of treatment. Amphotericin-B 3mg/kg/day was started with monitoring of galactomannan levels; based on the findings of high resolution computed tomography (HRCT) antibiotic therapy was switched to imipenem 500mg iv every 6h. Tigecycline 150mg iv every 12h was also added because of Gram-negative bacilli growth in subsequent three blood cultures. Despite that antibiotic modification, there was persistence of fever. Blood cultures grew Gram-negative bacilli, which were identified as “Raoultella ornithinolytica” by matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) (Bruker Biotyper) and confirmed by conventional biochemical tests. MICs of antibiotics were determined by BD Phoenix automated microbiological system (Becton Dickinson, Sparks, MD, USA). Amoxicillin–clavulanic acid 1g PO every 8h was then added to the regimen. Clinical response did not ensue and it was switched to ciprofloxacin 400mg iv every 12h according to the results of antibiotic sensitivity testing (Table 1). The patient was transferred to the intensive care unit where he died one week later.
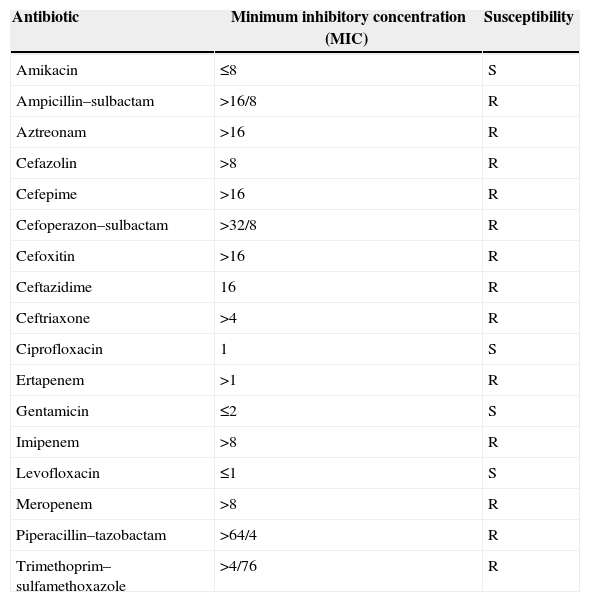
Susceptibility profile of Raoultella ornithinolytica.
| Antibiotic | Minimum inhibitory concentration (MIC) | Susceptibility |
|---|---|---|
| Amikacin | ≤8 | S |
| Ampicillin–sulbactam | >16/8 | R |
| Aztreonam | >16 | R |
| Cefazolin | >8 | R |
| Cefepime | >16 | R |
| Cefoperazon–sulbactam | >32/8 | R |
| Cefoxitin | >16 | R |
| Ceftazidime | 16 | R |
| Ceftriaxone | >4 | R |
| Ciprofloxacin | 1 | S |
| Ertapenem | >1 | R |
| Gentamicin | ≤2 | S |
| Imipenem | >8 | R |
| Levofloxacin | ≤1 | S |
| Meropenem | >8 | R |
| Piperacillin–tazobactam | >64/4 | R |
| Trimethoprim–sulfamethoxazole | >4/76 | R |
S, susceptible; R, resistant.
It should be kept in mind that Raoultella ornithinolytica can be the etiologic agent especially in patients with underlying conditions. One of the most important issues is the multidrug resistant profile of these bacteria. Ten to fourteen days of treatment with tigecycline, amoxicillin–clavulanic acid, levofloxacin, and cefmetazole are recommended in the literature.3–5 However, all of these drugs may fail in some cases, such as the patient herein reported.
Conflicts of interestThe authors declare no conflicts of interest.
