
A previously healthy 29-year-old male in intimate contact with dogs presented with a five-day history of high fever, chills, headache, myalgia and nonproductive cough. He also complained of sharp right-sided chest pain worse on deep inspiration. On physical examination, the patient was febrile, tachypneic and tachycardic. Inspiratory rales were heard over the right lower lung zone. Laboratory data showed a white blood cell (WBC) count of 6.6×109/L with a left shift. Inflammatory markers were mildly elevated with erythrocyte sedimentation rate (ESR) 37mm/h and C-reactive protein (CRP) 32mg/L. A computed tomography (CT) scan of the chest revealed a 3cm×3cm, well-defined and round mass surrounded by a halo of ground-glass attenuation, namely the halo sign, in the posterior basal segment of the right inferior lobe (Fig. 1). Serologic test was positive for Coxiella burnetii (C. burnetii) by indirect immunofluorescence assay (IFA). Empirical treatment was initiated with azithromycin (0.5g daily), which was changed to doxycycline (100mg twice a day) for 14 days. A follow-up CT scan performed four weeks later showed total resolution of the lesions. At six-month follow-up, the patient was asymptomatic with no radiological evidence of a relapse.
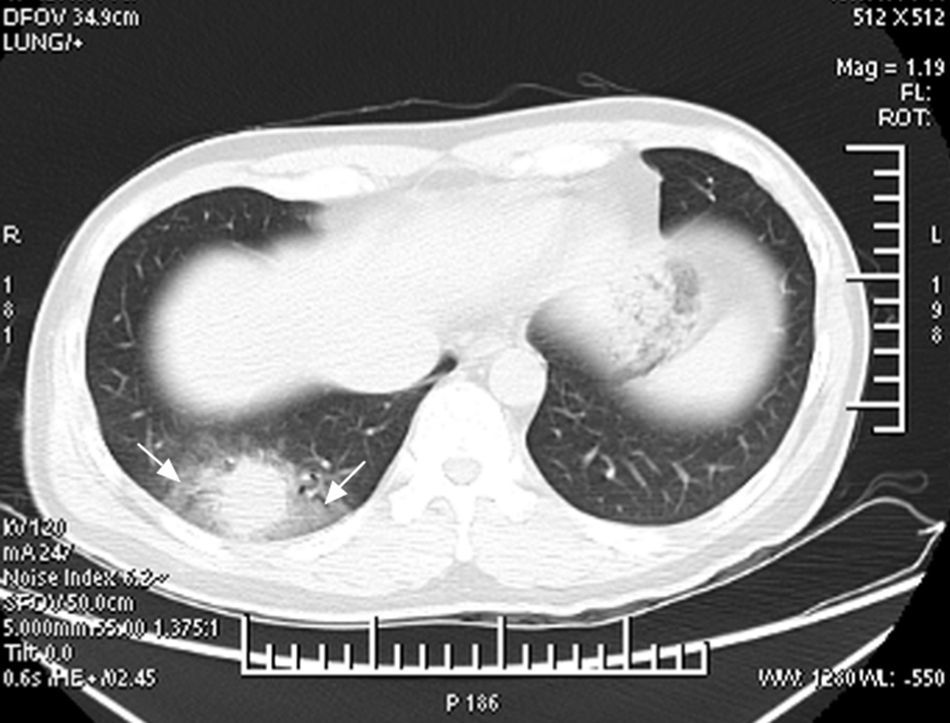
 scan of the chest showing a 3cm×3cm, well-demarcated and spherical mass in the posterior basal segment of the right inferior lobe surrounded by a wide zone of ground-glass opacities (arrows), the halo sign.")
Pneumonia is one of the cardinal manifestations of Q fever, which caused by C. burnetii infection.1 Q fever is probably the most common cause of round pneumonia in adults.2 The halo sign refers to a zone of ground-glass attenuation surrounding the circumference of a pulmonary nodule or mass on CT images.3,4 It has been attributed to hemorrhagic lesions mainly caused by an infectious process.1C. burnetii infection can exceptionally manifest with a halo sign, which is caused by the infiltration of inflammatory cells and exudates into the lung.4 Importantly, the halo sign is a useful diagnostic clue and may be good evidence of Q fever pneumonia.
Conflicts of interestThe authors declare no conflicts of interest.
This work was partly supported by the Medical Education Research Project of Shanghai Jiao Tong University School of Medicine (No. YB130910).
