
Invasive pneumococcal disease is a relevant public health problem in Brazil, especially among children and the elderly. In July/2010 a 10-valent pneumococcal conjugate vaccine was introduced to the immunization schedule of Brazilian children under two years of age. Between July/2010 and December/2013 we conducted a case-series study on invasive pneumococcal disease in Salvador, Brazil to describe the clinical and bacteriological profile of invasive pneumococcal disease cases during the post-implementation period. Eighty-two cases were eligible. Mean age was 31 years (interquartile range, 3–42); 17.1% and 30.5% were under 2 years and 5 years, respectively. Pneumococcal meningitis (n=64, 78.1%), bacteraemic pneumococcal pneumonia (n=12, 14.6%) and bacteraemia (n=6, 7.3%) were the clinical syndromes identified. Thirty-three different serotypes were found. Of these, serotype 14 (n=12, 14.6%) was the most common, followed by 23F (n=10, 12.2%), 12F (n=8, 9.8%), 18C (n=5, 6.1%) and 6B (n=5, 6.1%). Investigations conducted in Salvador in the pre-vaccine period did not identify serotype 12F as one of the most prevalent serotypes. Increase of serotype 12F was observed in different regions of Brazil, in the post-vaccine period. Among children under two years of age, the target group for 10-valent pneumococcal conjugate vaccine, 11 (78.6%) of the 14 isolated strains of Streptococcus pneumoniae belonged to vaccine serotypes; at least 50% of these children were not vaccinated. The relatively recent implementation of 10-valent pneumococcal conjugate vaccine in Brazil reinforces the need to maintain an active surveillance of invasive pneumococcal disease cases, considering the possible increase of invasive pneumococcal disease cases related to non-vaccine serotypes and the changes on the clinical presentation of the disease.
Streptococcus pneumoniae is a major cause of meningitis, bacteraemic pneumonia and sepsis,1 accounting for significant morbidity and mortality rates worldwide.2 Invasive pneumococcal disease (IPD) is a relevant public health problem in Brazil, especially among children and the elderly.3 In the decade before the implementation of 10-valent pneumococcal conjugate vaccine (PCV10), S. pneumoniae was responsible for 12% of bacterial meningitis in Brazil among children aged under two years and older and adults.4
Pneumococcal 7-valent conjugate vaccine (PCV7) was licensed in the United States in 2000 and accounted for significant reduction in incidence and mortality from IPD in the US.5 A study conducted in the US presented evidence that the vaccine provides herd immunity.5 However, follow up of IPD in the same country revealed an increased incidence of invasive disease caused by serotypes not included in PCV7 specially 19A,6 a phenomenon named replacement. Serotype replacement led to the development of vaccines with larger serotype coverage,7 which are currently available.
In Brazil, PCV7 was incorporated into the National Immunization Program in 2002, available only to children under five years of age at high risk of pneumococcal diseases.8 In July 2010 PCV10 was introduced to the immunization schedule of Brazilian children under two years of age.9 In addition to the conjugate vaccines, pneumococcal 23-valent polysaccharide vaccine (PPV23) is offered for individuals over two years of age at high risk of pneumococcal disease.8
Initial evaluation of IPD after PCV10 implementation in Brazil was published in 2013. A significant reduction in incidence of IPD caused by vaccine serotypes was observed among children under two years of age in the São Paulo University Hospital.10 In the same study, there was no significant change in incidence of IPD caused by non-vaccine serotypes. Declines in hospitalizations rates for pneumonia were found in three major cities in Brazil in the year 2011.11 A short period of observation after implementation of PCV10, however, was emphasized as a limitation in both studies.
The surveillance of IPD and the recognition of serotypes that cause greater morbidity and mortality are essential to assess the effectiveness of the immunization programs.12,13 Additionally, the vaccine status and presence of comorbidities play a role on the occurrence of IPD. Documentation of IPD cases is insufficient in developing countries.14 Given the lack of data on IPD in the post-vaccine period in Brazil, there is a strong need for more studies on the clinical presentation of the disease and profile of invasive strains. In this regard, the objective of this study was to describe the clinical and bacteriological profile of IPD cases diagnosed between July 2010 and December 2013 in Salvador, Brazil, through case-series study on IPD.
Material and methodsThis was a retrospective observational study, with a prospective component. Between July 2010 and December 2013 we conducted a case-series study on IPD in Salvador, Brazil, involving the Hospital Couto Maia (HCM), the Paediatric Centre Professor Hosannah de Oliveira (CPPHO) and the Cerebrospinal Fluid Laboratory (SINPEL). HCM is the referral hospital for infectious diseases in the state, mainly for the public health care system; CPPHO is the pediatric unit of the Federal University of Bahia Hospital; SINPEL performs cerebrospinal fluid (CSF) analysis of patients seen in the supplementary health care system in the city of Salvador. IPD cases were defined by the isolation of pneumococcus from a normally sterile site (blood or CSF). Patients with diagnosis of IPD with positive CSF or blood cultures for S. pneumoniae in HCM, CPPHO or SINPEL, between July 2010 and December 2013 were included in the study. Patients for whom it was not possible to obtain contact information were excluded.
Samples of blood or CSF for culture were obtained from patients with clinical suspicion of IPD, according to the routine of the centers involved. Based on the record of positive cultures for S. pneumoniae, isolates were sent to the Pathology and Molecular Biology Laboratory of the Research Centre Gonçalo Moniz CPqGM/FIOCRUZ for confirmation. Identification of S. pneumoniae was performed using standard bacteriological techniques, including Gram stain, colony morphology on agar media with 5% of sheep blood, optochin susceptibility (5μg Oxoid disks) and bile solubility.
Serotyping was performed by multiplex-PCR as described elsewhere.15,16 The isolates with negative or equivocal results in multiplex-PCR were sent to Adolfo Lutz Institute (National Reference Laboratory, Ministry of Health) and subjected to Quellung reaction for definition of capsular serotype. All isolates identified as serogroup 6 was subjected to wciN6C-specific PCR, for the identification of potential serotype 6C and 6D isolates.17
Clinical and demographic data (age, date of admission and diagnosis) were collected by review of the medical charts or from the data recorded on the request of cultures to laboratories. Patients were contacted by telephone and asked to e-mail photo of vaccination card to confirm the use of pneumococcal vaccine prior to the episode of IPD.
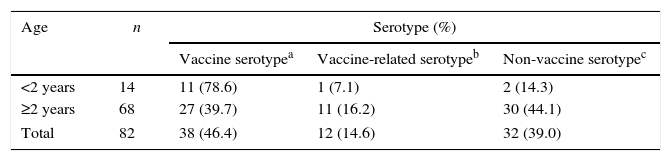
Vaccine serotypes are those included in PCV10 (1, 4, 5, 6B, 7F, 9V, 14, 18C, 19F and 23F); vaccine related serotypes (6A, 6A/B/C, 6C, 7C, 9L/N, 9N, 18B, 19A, 23B) were defined as those not included in PCV10, but sharing the same serogroup with the vaccine serotypes; other serotypes were considered non-vaccine types.
Collected data were entered and analyzed in the program SPSS version 17. For description, proportions of categorical variables and measures of central tendency and dispersion of continuous measurements are presented.
This project was approved by the Ethics Committee of the Federal University of Bahia School of Medicine.
Results and discussionDuring the period from July 2010 through December 2013, 93 cases of IPD were identified. Of these, 11 (11.8%) were excluded because of the unavailability of clinical, epidemiological and contact information, resulting in 82 patients, which comprise the study sample. Ten different serotypes (12F, 18B, 7F, 4, 23F, 6A, 22F, 6B, 34 and 28A) were isolated from individuals excluded from the study. Of these 11 excluded isolates, 4 (36.4%) belonged to vaccine serotypes, 3 (27.3%) belonged to vaccine-related serotypes and 4 (36.4%) belonged to non-vaccine serotypes. Capsular serotypes, age information and information on clinical syndrome of pneumococcal disease were obtained for all 82 cases of IPD.
Mean age was 31 years (interquartile range, 3–42). Twenty-five cases (30.5%) occurred in patients aged less than 5 years. Of these, 14 (56%) children were under 2 years of age. In Brazil, it was observed predominance of children under two years among cases of IPD pre and post-PCV10 implementation.9,18 In this context, the introduction of pneumococcal conjugate vaccines, which confer serotype-specific immunity to children under two years of age, is an important strategy for the prevention of IPD in Brazil.
Pneumococcal meningitis (n=64, 78.1%), bacteraemic pneumococcal pneumonia (n=12, 14.6%) and bacteraemia (n=6%, 7.3%) were the clinical syndromes identified. An international surveillance system of IPD in Latin America also identifies predominance of meningitis in Brazil, during the pre-vaccine period.19 Nevertheless, it is established that among IPD, pneumonia incidence is higher than that of meningitis.1 In Brazil, blood culture collection is recommended only for severe cases of pneumonia, when patients are hospitalized.20 In contrast, in Brazil meningitis cases should be notified and all suspected cases of meningitis must be submitted to blood culture collection and cerebrospinal fluid collection for culture, unless a contraindication exists.21 It is possible that the incidence of pneumococcal pneumonia in Brazil is underestimated as a consequence of these recommendations, resulting in the preponderance of meningitis observed in this study.
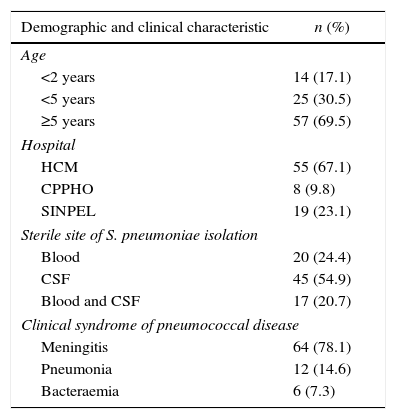
Pneumococcus strains were isolated exclusively from CSF in 45 cases (54.9%), exclusively from blood in 20 cases (24.4%) and from both blood and CSF in 17 cases (20.7%). Demographic and clinical characteristics of the study sample are shown in Table 1.
Demographic and clinical characteristics of 82 cases of invasive pneumococcal disease in Salvador, Brazil, from July 2010 through December 2013.
| Demographic and clinical characteristic | n (%) |
|---|---|
| Age | |
| <2 years | 14 (17.1) |
| <5 years | 25 (30.5) |
| ≥5 years | 57 (69.5) |
| Hospital | |
| HCM | 55 (67.1) |
| CPPHO | 8 (9.8) |
| SINPEL | 19 (23.1) |
| Sterile site of S. pneumoniae isolation | |
| Blood | 20 (24.4) |
| CSF | 45 (54.9) |
| Blood and CSF | 17 (20.7) |
| Clinical syndrome of pneumococcal disease | |
| Meningitis | 64 (78.1) |
| Pneumonia | 12 (14.6) |
| Bacteraemia | 6 (7.3) |
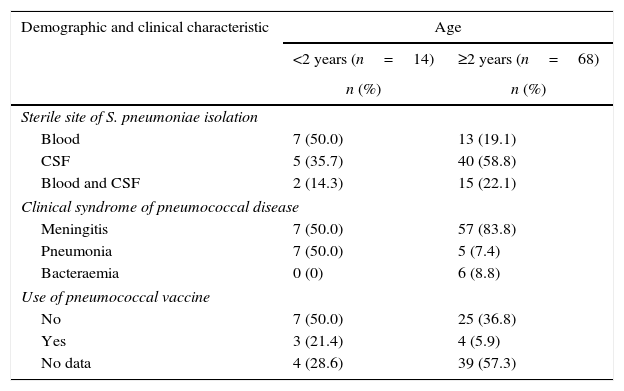
Information on use of pneumococcal vaccine was available in 39 cases. Of the 82 patients, 9 could not be contacted due to change of telephone number or address and 8 declined to inform. Among the 14 children under 2 years of age, the target group for PCV10, 3 (21.4%) had received PCV10 prior to the episode of IPD. Of these three children, only one had received an appropriate number of PCV10 doses for age (a total of 4 doses) and the other two children had received a single dose of PCV10. Three serotypes were isolated (3, 6B and 9L/N) from children under two years of age who were vaccinated. Serotype 3 was isolated from the child who had received an appropriate number of PCV10 doses. Among the 68 patients aged two years and above, 4 (5.9%) were vaccinated; of these, two children received PCV10 and the remaining two patients received PPV23. Serotypes 6B and 14 were isolated from the two children aged two years and above who received PCV10; both had received a single dose of PCV10. Serotypes 6C and 13 were isolated from patients who received PPV23. The patients who received PPV23 were adults and had indication for PPV23 vaccination based on their comorbidities: one was an individual with HIV infection and the other one was an individual with cerebrospinal fluid leaks. The patients with comorbidities are those who received PPV23. Demographic and clinical characteristics of study sample, stratified by age at diagnosis are shown in Table 2.
Demographic and clinical characteristics of 82 cases of invasive pneumococcal disease in Salvador, Brazil, from July 2010 through December 2013, stratified by age at diagnosis.
| Demographic and clinical characteristic | Age | |
|---|---|---|
| <2 years (n=14) | ≥2 years (n=68) | |
| n (%) | n (%) | |
| Sterile site of S. pneumoniae isolation | ||
| Blood | 7 (50.0) | 13 (19.1) |
| CSF | 5 (35.7) | 40 (58.8) |
| Blood and CSF | 2 (14.3) | 15 (22.1) |
| Clinical syndrome of pneumococcal disease | ||
| Meningitis | 7 (50.0) | 57 (83.8) |
| Pneumonia | 7 (50.0) | 5 (7.4) |
| Bacteraemia | 0 (0) | 6 (8.8) |
| Use of pneumococcal vaccine | ||
| No | 7 (50.0) | 25 (36.8) |
| Yes | 3 (21.4) | 4 (5.9) |
| No data | 4 (28.6) | 39 (57.3) |
Thirty-three different serotypes were found. Of these, serotype 14 (n=12, 14.6%) was the most common, followed by 23F (n=10, 12.2%), 12F (n=8, 9.8%), 18C (n=5, 6.1%) and 6B (n=5, 6.1%). Serotype 14 was also predominant in two studies conducted during the pre-vaccine period.18,22 In these studies, the most prevalent non-vaccine serotypes were 3 and 6A, and the conjugate pneumococcal vaccines are believed to provide cross-protection to serotype 6A.23 Unlike the present study, in previous investigations conducted in Salvador serotype 12F was not observed as one of the most prevalent serotypes.18,22 Surveillance of IPD cases in post-vaccine period is essential to determine the influence of serotype replacement after pneumococcal vaccination on the increase of serotype 12F, considering that cyclical changes in the incidence of serotypes may be responsible for this increase.24 Serotype 12F was observed as one of the most common serotypes in the post-vaccine period, in different regions of Brazil.10,25 This raises the possibility of current emergence of this serotype.
Among children under two years of age, eight serotypes were isolated. Of these, serotype 14 (n=4; 28.6%) was the most common. In this age group, most (78.6%) of the 14 strains belonged to vaccine serotypes, except serotypes 11A/D, 3 and 9L/N, with one isolate each. The elevated frequency of cases involving vaccine-serotypes among children under two years of age after the universal implementation of PCV10 may be partly explained by the low vaccine uptake in the study sample, in which at least 50% of children were not vaccinated. Of the 14 cases of IPD in children younger than two years, 11 (78.6%) occurred during the first year of implementation of PCV10. During this period, PCV10 was a newly implemented vaccine and therefore unknown to the population. It was necessary that those responsible for children were instructed by health professionals about the need of pneumococcal vaccination and the vaccine availability. This implementation period may explain the low vaccine uptake among children under two years of age in the study sample.
Thirty-one different serotypes were isolated from individuals two years of age and above. Of these, 14 (n=8, 11.8%), 12F (n=8, 11.8%) and 23F (n=8, 11.8%) were the most common. In this age group, most isolates (n=30, 44.1%) belonged to non-vaccine serotypes, a pattern similar to that reported during the pre-vaccine period.22 The serotype distribution according to the inclusion in PCV10 is described in Table 3.
Distribution of capsular serotypes of S. pneumoniae isolated from cases of invasive pneumococcal disease from July 2010 through December 2013 according to the inclusion in PCV10.
Considering all age groups, the most frequent serotypes isolated from blood were 14 (n=6, 30%), 6B (n=4, 20%) and 19A (n=2, 10%). From CSF, 23F (n=9, 20%), 12F (n=6, 13.3%) 14 (n=4, 8.9%) and 18C (n=4, 8.9%) were the most prevalent. Diversity in distribution of pneumococcal serotypes according to the sterile site of isolation is also described by other authors and it is probably a consequence of individual characteristics of each serotype.26 Foster and colleagues reported that serotype 12F significantly increases the risk of meningitis compared to other IPD.27 In this study, the serotype 12F was the second most prevalent among those isolated from CSF.
This study is based on a non-probability sampling and therefore it is possible that some results presented here are an outcome of selection bias. A case-series, however, is an appropriate study design to describe the clinical and bacteriological characteristics of IPD, the main objective of this investigation.
The relatively recent implementation of PCV10 in Brazil reinforces the need to maintain an active surveillance of IPD cases. Maintaining surveillance of IPD in Salvador is critical to clarify the role of PCV10 in changes on serotypes incidence, considering the possible increase of IPD cases related to non-vaccine serotypes.
Conflicts of interestThe authors declare no conflicts of interest.
We thank the professionals of Hospital Couto Maia, Paediatric Centre Professor Hosannah de Oliveira and Cerebrospinal Fluid Laboratory; and the patients and their families.
