

Drug shortages pose a clear detriment to antimicrobial stewardship (AS) efforts. Our objective was to evaluate the effect of a piperacillin-tazobactam shortage on meropenem use, related costs, and associated changes in AS activity. A quasi-experimental quality improvement review compared adult patients receiving meropenem ≥72h three months pre-shortage and three months during the shortage. 320 patients were included (pre-shortage: 103; shortage: 217). Baseline characteristics were similar, but the length of stay was slightly longer in pre-shortage [19 (11–32) days] versus shortage [16 (11–32) days] (p=0.094). In pre-shortage and shortage, median days of therapy and estimated meropenem cost were 7 (5–11) and 7 (5–10) and $309.93 ($173.60–$507.03) and $255.30 ($204.24–$424.31), respectively (p=0.411 and p=0.050). Frequency of ID consultation was similar (16.8% in pre- and 25.3% in shortage, p=0.091). AS interventions increased during the shortage period (99 in pre-shortage and 205 in shortage). De-escalation occurred in 19.4% versus 32.7% of the patients in pre-shortage and shortage (p=0.014). The piperacillin-tazobactam shortage was associated with a 111% increase in meropenem prescriptions despite active AS, but was not associated with changes in mortality, length of therapy, or meropenem costs. AS should be aware that shortages may require proactive countermeasures to avoid inappropriate antimicrobial use during shortage periods.
According to the American Society of Health-Systems Pharmacists (ASHP), a drug shortage is defined as “a supply issue that affects how a pharmacy prepares or dispenses a drug or product that influences patient care such that a prescriber must use an alternative agent”.1 From 2007 to 2011, the numbers of new and ongoing drug shortages, including anti-infectives, increased.2,3 As a result, the Food and Drug Administration developed a strategic plan intended to prevent and mitigate drug shortages.4,5 Additionally, the Generating Antibiotic Incentives Now (GAIN) and Antibiotic Development to Advance Patient Treatment (ADAPT) Acts were established in 2012 and 2013, respectively, to provide incentives, including fast-track approval, to add new anti-infectives to the market. Although the number of new drug shortages has begun to decline since 2011, approximately 300 drugs annually remain on active/ongoing shortages.6 Shortages affecting antimicrobial agents, including those used for acute, life-threatening illnesses, present some of the largest challenges for clinicians.
With infections caused by Gram-negative pathogens on the rise, our antimicrobial stewardship program (ASP) sought to preserve meropenem usage for patients with an ASP-deemed appropriate indication (infection with or history of infection with extended-spectrum beta-lactamase-producing organism or an organism resistant to third-generation cephalosporins, clinical/microbiological treatment failure requiring escalation). Through implementation of this targeted stewardship audit and feedback intervention, meropenem usage declined by more than 30% (unpublished data). In the first quarter of 2015, however, piperacillin-tazobactam went on shortage. Therefore, the objective of this study was to determine the impact of a piperacillin-tazobactam shortage on the usage of meropenem, clinical and economic outcomes, and associated ASP activities.
This quasi-experimental quality improvement retrospective review was conducted at a large academic medical center (700+ beds) as part of routine antimicrobial stewardship efforts in compliance with Institutional Review Board requirements. A convenience sample of meropenem utilization three months prior to the ASHP-denoted national shortage of piperacillin-tazobactam was compared to meropenem use during the three months during the shortage. A one month washout period in which the stock of piperacillin-tazobactam was depleted occurred in January. Patients were identified using TheraDoc Clinical Surveillance Software (Premier, Inc.; Salt Lake City, UT). Data were collected from patient charts using the EPIC Systems electronic charting system (Madison, WI). All adult patients that received ≥72 consecutive hours of meropenem therapy were included. Patients less than 18 years of age, those who died within 72h of therapy initiation, or duplicate patients (hospitalizations other than the first within the time period) were excluded. Demographic characteristics and medication allergy information were collected for each patient. Information regarding hospital course, including length of stay, location (intensive care unit at any time during receipt of meropenem vs. ward), in-hospital mortality, 30-day readmission, and whether an infectious disease (ID) consult occurred, were collected. Dose, duration, and frequency of meropenem administration, along with comorbidities, indication for meropenem treatment, and adverse drug reactions were collected. Any cultured organisms were recorded, along with culture source. We also recorded whether de-escalation to another beta-lactam was possible (based on timing of culture results) and whether de-escalation occurred. Finally, total number of documented interventions of ASP activity, including chart review prompted by targeted drug alerts, antimicrobial de-escalation or antimicrobial dosage/frequency changes during these time frames were also recorded. ASP interventions were irrespective of ID consultation and recommendations from either do not routinely overlap.
The primary outcomes were meropenem usage rates, clinical (mortality, length of stay and ICU status) and meropenem-related cost analysis, and associated ASP activities in each period. Secondary outcomes included number of infectious diseases consults and prescribing trends based upon resistance. Categorical data was analyzed utilizing Chi-square or Fisher's Exact tests. Mann–Whitney U and Student's t-test were performed for continuous data. All statistical analyses were performed using SPSS Statistical Software (Release 22, SPSS, Inc., Chicago, IL, USA). A p-value ≤0.05 was considered statistically significant.
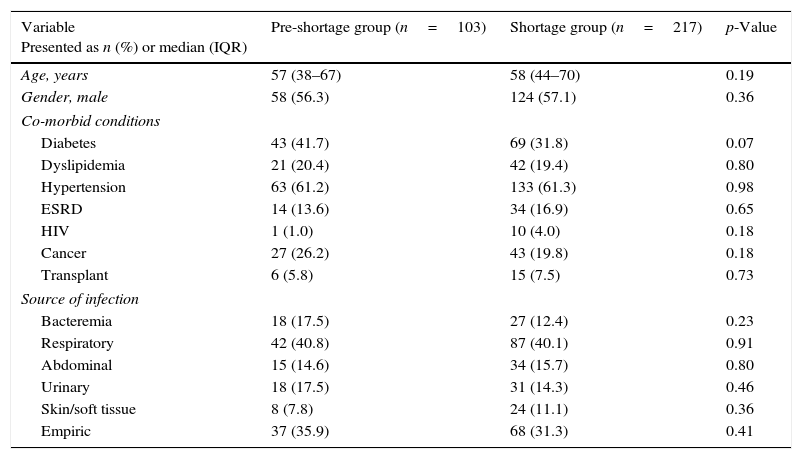
A total of 771 charts were screened for review. After excluding 451 patients (10 patients <18 years old, 169 <72h of consecutive meropenem therapy, 272 duplicate patients), 320 patients were included in this study, with 103 in the pre-treatment group and 217 in the shortage group. The median (IQR) age of the cohort was 57 (43–68) years of age. Gender was predominately male (56.9%) and the majority of the patients were African American (57.0%). Baseline characteristics and demographics were similar between the two groups, with the most common comorbid conditions being hypertension and diabetes (Table 1). A dramatic 111% increase in meropenem usage was observed from the pre-shortage to shortage arms. Overall, no mortality difference was observed between the pre-shortage and shortage groups (24.3% and 22.6%, respectively (p=0.74)). Intensive care unit (ICU) status was comparable in both arms, with ICU admittance representing 62.8% of the population. In the pre-shortage group, median length of stay was statistically longer than in the shortage group (p=0.02) (Table 2). The median (IQR) days of therapy between groups was comparable at 7 (5–11) and 7 (5–10) days, respectively (p=0.411). ID consultation was performed in 16.8% and 25.3% of the patients in the pre- and shortage arms (p=0.091) with increased de-escalation occurring in the shortage patients (19.4% vs 32.7%, respectively (p=0.014)). The most frequently utilized antimicrobial classes upon de-escalation in either group were the fluoroquinolones and beta-lactams. Overall, estimated median meropenem cost per patient, despite no difference in dosing, was $309.93 ($173.60–$507.03) and $255.30 ($204.24–$424.31) in the pre- and shortage groupings (p=0.05). While many isolates were collected, the predominant pathogens identified were Escherichia coli (30.6%), Klebsiella pneumoniae (16.3%) and Enterobacter spp. (10.0%) for both groups. The pre-shortage group had a higher frequency of patients with multiple pathogens isolated (17.5% vs. 8.8%), increased frequency of ESBL organisms (17.5% vs. 6.5%), and decreased opportunity for de-escalation (75.5% vs. 88.5%). Overall ASP interventions increased during the shortage period (99 in pre-shortage and 205 in shortage).
Patient demographics.
| Variable Presented as n (%) or median (IQR) | Pre-shortage group (n=103) | Shortage group (n=217) | p-Value |
|---|---|---|---|
| Age, years | 57 (38–67) | 58 (44–70) | 0.19 |
| Gender, male | 58 (56.3) | 124 (57.1) | 0.36 |
| Co-morbid conditions | |||
| Diabetes | 43 (41.7) | 69 (31.8) | 0.07 |
| Dyslipidemia | 21 (20.4) | 42 (19.4) | 0.80 |
| Hypertension | 63 (61.2) | 133 (61.3) | 0.98 |
| ESRD | 14 (13.6) | 34 (16.9) | 0.65 |
| HIV | 1 (1.0) | 10 (4.0) | 0.18 |
| Cancer | 27 (26.2) | 43 (19.8) | 0.18 |
| Transplant | 6 (5.8) | 15 (7.5) | 0.73 |
| Source of infection | |||
| Bacteremia | 18 (17.5) | 27 (12.4) | 0.23 |
| Respiratory | 42 (40.8) | 87 (40.1) | 0.91 |
| Abdominal | 15 (14.6) | 34 (15.7) | 0.80 |
| Urinary | 18 (17.5) | 31 (14.3) | 0.46 |
| Skin/soft tissue | 8 (7.8) | 24 (11.1) | 0.36 |
| Empiric | 37 (35.9) | 68 (31.3) | 0.41 |
In this study, a piperacillin-tazobactam shortage was associated with a 111% increase in meropenem prescriptions despite active antimicrobial stewardship, but was not associated with changes in mortality, length of therapy, or meropenem costs. During the shortage period, ASP interventions and ID consults increased and ESBL rates decreased. There was no difference in in-hospital mortality or length of meropenem therapy between the pre-shortage and shortage groups. However, in the pre-shortage group, length of stay and meropenem drug costs were numerically higher. This may be attributable to the increased number of resistant organisms or the increased length of stay in this period. In the shortage group, ID was consulted more often and the ASP recorded more than twice the number of overall interventions. The increased ASP presence during the shortage period may be responsible for the increase in de-escalation.
In a study of the impact of a 2002 piperacillin-tazobactam shortage on antimicrobial prescribing rates, Mendez and colleagues found that, while piperacillin-tazobactam use decreased, ceftriaxone, levofloxacin, metronidazole, ampicillin-sulbactam, and ticarcillin-clavulanate use increased.7 Although this study did a thorough job evaluating the impact of an antimicrobial shortage on other agents, carbapenem usage rates were variable depending on the analysis used (slight decrease by charged dose, slight increase by gram usage). This is in contrast to our findings of a significant increase in carbapenem usage (by number of prescriptions) during the shortage period.
In a similar study, Pluss-Suard and colleagues evaluated changes in broad-spectrum antibiotics following a cefepime shortage.8 Investigators found significant increases in piperacillin-tazobactam and meropenem in hospitals with definitive and transient interruptions in cefepime supply, respectively, and associated significant increases in overall cost. Similar to these investigators, we found that, in the midst of a piperacillin-tazobactam shortage, our meropenem rates increased. In contrast to this study, though, our meropenem drug costs were lower during the shortage period. This may be due to the diligence and increased de-escalation efforts of our ASP.
Finally, in a study of the impact of an intravenous trimethoprim/sulfamethoxazole shortage on treatment outcomes with Pneumocystis jirovecii pneumonia, Dilworth and colleagues found that more patients experienced treatment failure, worsening clinical status, and had slightly longer length of stay during the shortage as compared to the pre-shortage period.9 It was suggested that, although the negative impact on patient outcomes was immediate, collaboration between pharmacists and physician caregivers improved outcomes and lessened the global impact of the shortage. The patient outcomes in this study are in contrast to our finding of a significantly decreased length of stay during the pre-shortage group and the findings of no difference between groups in length of therapy, days of therapy, and ICU status. However, the increase in ASP interventions and ID consults in our study are likely similar to Dilworth's reported collaboration between pharmacists and physicians, which may be responsible for the overall similarity between outcomes in our evaluated groups.
Other institutions have also seen benefit of collaboration between healthcare providers, suggesting that combined efforts are needed to address and sufficiently respond to drug shortages.9,10 Without the diligence and pre-emptive activity by our ASP, the impact of the piperacillin-tazobactam shortage on meropenem use at this institution may have been more drastic. Moving forward, hospitals should consider having a shortage-response plan in place, similar to the concept of disaster management plans many hospitals utilize. Concepts such as our EPIC alternative therapy pop-up, automatic alternative substitution by the pharmacy department, and prescriber education may also be beneficial. In the case of antimicrobial shortages, the involvement of an antimicrobial stewardship program is essential to protect the welfare of the patient while deciding how best to allocate the shorted medications.
Similar to the challenges with infection control and containment in developing or low-income countries,11,12 antimicrobial shortages may present challenges for appropriate management of infections in these regions. Similar to the challenge of containing Ebola that was seen in Africa recently,12 a lack of specific treatments and reliable interventions in resource-poor countries, including those instigated by an antimicrobial shortage, may be highly impactful for patient care. Antimicrobial stewardship efforts to substitute the most appropriate available therapies, even without a formal ASP, should be undertaken in these situations in order to lessen the impact on clinical outcomes.
As with other retrospective quasi-experimental reviews, our study is not without limitations. First, inclusion criteria included meropenem use for 72h, which does not account for courses of meropenem on which the ASP intervened at 24 or 48h. Next, although we know that piperacillin-tazobactam use in the shortage period was negligible, use in the pre-shortage period was not monitored by the ASP or recorded. In addition, usage rates of other comparable broad-spectrum regimens on formulary (cefepime or ceftriaxone plus metronidazole) were not obtained for either period. Finally, culture data were recorded for the individual patients included, but resistance data for the institution as a whole (carbapenem-resistant enterobacteriaceae, Clostridium difficile, vancomycin-resistant enterococci) are not available for these periods. Lastly, we only report bivariate analyses. Therefore, the effects related to unique populations such as oncologic or ICU admitted patients may be diluted by the overall population.
Antimicrobial shortages have an impact on the prescribing habits of clinicians irrespective of an established ASP. Although meropenem use increased dramatically during the piperacillin-tazobactam shortage period, ASP interventions, ID consults, and overall de-escalation also increased, mortality rates and length of therapy remained consistent, and average meropenem cost per course decreased. With the potential for adverse clinical outcomes associated with these shortages, hospitals should consider more aggressive, alternative strategies to avoid inappropriate antimicrobial usage during these times.
Conflicts of interestThe authors declare no conflicts of interest.
No specific funding was received for this work. The authors have not received any financial reimbursement from any pharmaceutical companies for any of the work presented in this article. The authors do not own any stocks or shares relevant to this study, nor has any funding agency been involved in the study design. No professional medical writers have been involved in this manuscript preparation, and no reimbursement has been received for preparation of this article.
