
To test the validity of the polymerase chain reaction for diagnosing American visceral leishmaniasis, 88 suspected cases were studied. Diagnosis was confirmed in 47 (53.5%) and ruled out in 41 (46.5%) patients. Samples of bone marrow and peripheral blood were processed by polymerase chain reaction to evaluate the sensitivity and specificity of the test and its agreement beyond chance with microscopy examination. The polymerase chain reaction was positive in bone marrow of 100% of the patients with amastigotes seen with microscopy examination, and in 59.5% in those where no parasite were seen. Agreement beyond chance between visualization of the parasite in bone marrow aspirates and polymerase chain reaction was considered weak (Kappa=0.41). Concordance between polymerase chain reaction of bone marrow aspirates and of peripheral blood was considered excellent (Kappa=0.88). The test turned out positive in all bone marrow aspirates of those with the disease and whereas the positivity rate was 58.5% among those without the disease, with specificity rate of 41.5%.
Clinicians who work in areas where American visceral leishmaniasis (AVL) is endemic are not always able to diagnose the cases due to regional concurrence of other diseases with similar manifestations. Definitive diagnosis is made by the identification of the parasites in tissue aspirates, either spleen or bone marrow. Spleen aspirate yield higher percentage of positivity but, due to bleeding risks, the bone marrow aspirate is more frequently used, despite having lower sensitivity.1 Parasite identification tests are invasive and uncomfortable, require trained personnel and a negative result do not rule out AVL diagnosis. Studies have shown polymerase chain reaction (PCR) to be both highly specific and sensitive for the diagnosis of visceral leishmaniasis.2–7 These studies compared people with confirmed AVL diagnosis to healthy persons, fitting Type II Study Classification of Sacket and Haynes.8 The purpose of the present study was to test the validity of PCR in a group of patients with clinical suspicion of AVL. The PCR protocol described by Smyth et al.9 was used in this study because, at the time, it was the standard method for DNA sequencing of regional Leishmania chagasi.
Materials and methodsThe type of study carried out was the “diagnostic test validation”, corresponding to phase III of Sacket and Haynes8 classification. The study included patients with diagnostic hypothesis of AVL admitted to “Hospital Escola Dr. Hélvio Auto” (HEHA), Maceió, Alagoas, between April 2003 and March 2005.
Study populationThe “cases” consisted of persons originating from endemic regions, with fever for 14 or more days, pallor, hepatosplenomegaly, and with or without amastigotes of Leismania in bone marrow aspirate smears. For those with negative bone marrow aspirate, the inclusion criteria was the hematologic tests (pancytopenia) and favourable response to treatment.10 Patients diagnosed as having AVL were treated with meglumine antimoniate, except for those with intolerance to the first dose of the medication, who were switched to amphotericin-B. Cure was defined according to the following criteria established by the Brazilian Minister of Health (2003)10: resolution of fever, reduction of visceral size, hemoglobin and leukocyte count elevation, weight gain. The “non-cases”, although with some of the above-mentioned manifestations of the disease, did not fulfill all diagnostic criteria. The variables listed in the protocol were: sex, age, size of liver and spleen, PCR result, and visualization of amastigotes in bone marrow aspirate by microscopy.11 Informed consent was obtained from patients or their representatives. Laboratory tests were performed according to the protocol established by the World Health Organization11 and adopted by the Brazilian Ministry of Health.10
Laboratory examinationSamples of peripheral blood and bone marrow were collected in tubes with EDTA, kept at −20°C for future processing by PCR amplification. DNA was extracted from these samples using the GFX genomic blood DNA purification kit (Amersham Pharmacia Biotech) according to manufacture's instructions. The used primers: AJS3 (5′-GGGGGTGGTAAATAGG-3′) and DB8 (5′-CCAGTTTCCCGCCCCG-3′), amplifies a ~800-base pairs (bp) sequence of a specific kinetoplast DNA minicircle of Leishmania described elsewhere.9
PCR reactions were carried out in a total volume of 50μL of reaction mixture containing 4μL of extracted DNA, 0.3μM of the primers AJS3 and DB8 (Invitrogen, USA), 1.25μM of each dNTP (Ludwig Biotecnologia Ltda), 3.0mM MgCl2 (Ludwig Biotecnologia Ltda), 2.5U/μL Taq DNA Polymerase (Ludwig Biotecnologia Ltda), and water free of nuclease (Promega, Madison, WI, USA). The PCR conditions consisted of 3min at 95°C, followed by 35 cycles of denaturing at 95°C for 30s, annealing at 60°C for 30s, extension at 72°C for 30s and a final extension for 6min at 72° C. PCR products were submitted to electrophoresis in a 1.2% (w/v) agarose gel stained with ethidium bromide (4.0mg/μL) and identified by visualizing the bands of expected size under UV transilluminator. A negative extraction control was used to assure absence of contamination during DNA extraction process. A negative control containing distilled DNA free water was also used.
Data analysisSensitivity and specificity with the respective confidence intervals were estimated for PCR results using bone marrow aspirate and peripheral blood in relation to tissue microscopy. Concordance between PCR results in bone marrow and peripheral blood were assessed by Kappa statistic.12
ResultsThe study population consisted of 88 subjects, predominantly males (60.2%), below the age of 15 (55.7%), and of rural origin (64.8%). Of the total, 47 (53.4) were considered “cases” (46 positive for parasites in bone marrow and one negative), and 41 (46.6%) “non-cases”. The classification of subjects into “cases” and “non-cases” was made according to the diagnostic criteria already defined.
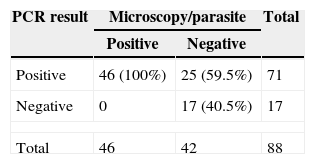
All blood samples were subjected to PCR. Tests were positive in 71 subjects. Concordance between amastigote demonstration by microscopy and PCR was considered weak (Kappa 0.21–0.40) (Table 1). Compared to bone marrow aspirate PCR showed high sensitivity, but low specificity for disease diagnosis.
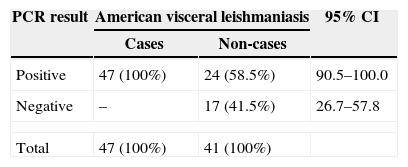
PCR in bone marrow aspirates tested positive in all AVL patients (cases) and in 24 (58.5%) of those who did not have active disease, indicating low specificity, as observed in Table 2.
PCR results in bone marrow aspirates of patients with and without American visceral leishmaniasis prior to treatment.
| PCR result | American visceral leishmaniasis | 95% CI | |
|---|---|---|---|
| Cases | Non-cases | ||
| Positive | 47 (100%) | 24 (58.5%) | 90.5–100.0 |
| Negative | – | 17 (41.5%) | 26.7–57.8 |
| Total | 47 (100%) | 41 (100%) | |
CI, confidence interval; PCR, polymerase chain reaction.
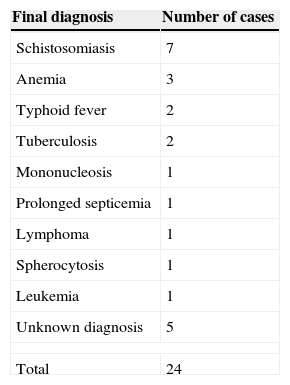
False positive cases, after the diagnosis of AVL was ruled out, were found to have a variety of other illnesses, as shown in Table 3.
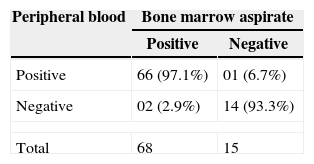
Bone marrow aspirates and peripheral blood samples obtained prior to treatment were evaluated by PCR. The agreement beyond chance was 0.88, a result considered excellent (Kappa=0.88–0.99) (Table 4). This indicates that peripheral blood examination could replace bone marrow aspirates due to better acceptance and facility of collection.
DiscussionIn this study patients with suspected diagnosis of AVL were young, 55.7% of them were under 15 years old. The same percentage of this age group was observed among those with confirmed AVL diagnosis. This result is comparable with those reported by Alves et al.13 for AVL cases in Brazil from 2000 to 2004.
Direct microscopic examination and/or culture of spleen aspirate are considered the gold-standard to confirm AVL diagnosis.14 Nevertheless, they are not recommended in endemic areas due to the potential of serious complications. The demonstration of Leishmania amastigotes in smears from lymph node and bone marrow aspirates, although less sensitive, is used as reference by health services in endemic areas.14 Several studies have demonstrated that PCR is highly sensitive and specific for leishmaniasis diagnosis.8,15,16 However, the majority of the authors compared PCR results between patients with AVL and healthy subjects, with the latter group coming from areas different from the former group. In this study the evaluation was made adjusting to phase III of Sacket and Haynes8 classification, which allows for a better judgment of the possible usefulness of the test for diagnostic purposes.
PCR results in bone marrow aspirates showed poor concordance assessed by the Kappa statistic with the detection of amastigotes by microscopy, despite its high sensitivity. The results observed in true positive patients on both diagnostic methods are in line with those obtained by Osman et al.5 and Salotra et al.7 These authors also reported elevated sensitivity of PCR in marrow blood aspirates, and concluded that PCR is as good as the search for parasites in lymph nodes or bone marrow in confirmed AVL cases. The low specificity observed diverges from the results of other authors like Piarroux et al.,6 Lachaud et al.3 and Disch et al.,16 who found 100% specificity. In their studies cases and controls were not from the same area.
Of the 25 subjects suspected of AVL with only positive PCR, 24 were diagnosed as not having leishmaniasis. The remaining patient had the diagnosis of AVL despite negative parasitological examination, on the grounds of epidemiological data, clinical presentation, hematological findings showing pancytopenia, and satisfactory treatment response.
Medical literature reports the existence of asymptomatic cases in endemic areas. In northeast Italy Pampiglione et al.17 demonstrated antibodies against Leishmania in 3.7% of the analyzed population. Six asymptomatic persons underwent liver biopsy, and in one of them amastigotes were found in liver tissue. In Brazil, Evans et al.18 evaluating children less than 11 years old, found 4.6% with antibodies against Leishmania. Caldas et al.19 in the same country found anti-Leishmania antibodies in 34.4% of children (ages 0–5), and Costa et al.20 found Leishmania kDNA in asymptomatic persons living in same households of AVL patients. More recently, Adini et al.21 identified 2.9% positive sera for anti-Leishmania antibodies in asymptomatic subjects residents of Israel. These studies suggest that AVL behaves like tuberculosis and Hansen's disease in regard to the number of infected subjects being much larger than the number of those having the disease. In the present study, cases and controls were from endemic regions, thus specificity findings are consistent with those by Fichoux et al.,22 Sharma et al.,23 and Lambson et al.24 The latter suggests that PCR is a convenient tool to detect asymptomatic carriers of the parasite in endemic areas.
The 17 individuals suspected of having AVL but with negative results on both tests were given other diagnosis. These subjects, if really exposed to the disease, reacted differently to the presence of the parasite. The outcome of infection seems to depend on a complex interaction of virulence factors of the parasite and host immunological mechanisms.25,26 As reviewed by Saha et al.,26 cellular immunity is crucial for susceptibility or resistance to leishmaniasis, but humoral response also seems to play a role. Parasite antigens do not induce delayed-type hypersensitivity with absence of lymphocyte proliferation, and inadequate production or secretion of interferon-gamma (IFN-gamma) and interleukin 2 (IL-2), citokynes related to the immune response.27 In the early stage of infection the IFN-gamma plays a role to control the infection.28 According to Jeronimo et al.29 cellular-mediated immunity is responsible for the spontaneous resolution of the infection and prevention of re-infections. Studies are also providing evidence that genetic risk factors contributes to the disease outcome.30 It is possible that the 17 subjects without infection had been exposed to the parasite but were immunologically competent, resisting effectively the development of the disease.
The false-negative PCR in the peripheral blood in the patient with parasites in the bone marrow microscopic examination could be due to: loss of the specimen at the time of the PCR test, time of the test, duration and conditions of specimen storage, presence PCR inhibitors in the blood, or periodicity of the circulating parasites.
Cutaneous tests, such as Montenegro reaction and search for antibodies, revealed that the infectious agent stimulates not only the cellular immunity but also the humoral, without flagging the presence of parasites in the patient. In contrast, a positive PCR, translate detection of specific DNA, meaning that the person harbors Leishmania amastigotes. This refers to AVL found in India and Sudan, where the reservoir and source of infection for the vector is the patient. Working in endemic regions of Brazil studies proved that AVL patients are infective to vectors.20,31 Although not yet proved, it is possible that asymptomatic carriers may serve as source of parasites to sand flies.
A limitation of this study was the fact that PCR was not done in all identified patients during the study period, which could lead to selection bias. To evaluate if this could compromise the validity of the study, comparison was made taking in consideration age, sex, average size of the liver and spleen: patients with AVL who had blood tested by PCR versus those whose blood was not tested, and patients without AVL but with PCR positive versus those with PCR negative. This analysis did not show significant differences (data not presented). It is believed that the inclusion of these subjects would not substantially change the results.
ConclusionThe present study used PCR to evaluate persons suspected of having AVL, answering questions formulated in phase III by Sacket and Haynes8 classification. The positivity rate found was higher in bone marrow aspirates and peripheral blood of patients diagnosed by microscopic examination. The test was also positive in patients without the disease but living in endemic regions (false-positive). Therefore, PCR should not be valued when used alone for diagnosis. However, it can be used as an ancillary diagnostic test in persons with strong indication of having the disease but with negative bone marrow aspirate, having the advantage to be performed in peripheral blood samples. It is also possible to use PCR to assess the prevalence of infection in specific population groups, and to evaluate the animal reservoir and vectors involved in the epidemiological chain.
Conflict of interestAll authors declare to have no conflict of interest.
The authors wish to thank all the patients for their willingness to participate in this study, and express gratitude to Maria de Fátima Thomas, MD, MPH, for assisting with translations and expert advice regarding research publication.
