
Patients submitted to hemodialysis are at a high risk for healthcare-associated infections (HAI). Presently there are scarce data to allow benchmarking of HAI rates in developing countries. Also, most studies focus only on bloodstream infections (BSI) or local access infections (LAI). Our study aimed to provide a wide overview of HAI epidemiology in a hemodialysis unit in southeastern Brazil. We present data from prospective surveillance carried out from March 2010 through May 2012. Rates were compared (mid-p exact test) and temporally analyzed in Shewhart control charts for Poisson distributions. The overall incidence of BSI was 1.12 per 1000 access-days. The rate was higher for patients performing dialysis through central venous catheters (CVC), either temporary (RR=13.35, 95% CI=6.68–26.95) or permanent (RR=2.10, 95% CI=1.09–4.13), as compared to those with arteriovenous fistula. Control charts identified a BSI outbreak caused by Pseudomonas aeruginosa in April 2010. LAI incidence was 3.80 per 1000 access-days. Incidence rates for other HAI (per 1000 patients-day) were as follows: upper respiratory infections, 1.72; pneumonia, 1.35; urinary tract infections, 1.25; skin/soft tissues infections, 0.93. The data point out to the usefulness of applying methods commonly used in hospital-based surveillance for hemodialysis units.
Patients with end-stage renal disease (ESRD) undergoing hemodialysis are especially prone to acquiring healthcare-associated infections (HAI).1 This is due to both the dialysis procedure and to the immune compromising effects of the underlying disease.2 However, like all HAI, those happening in hemodialysis patients can be prevented with the implementation of infection control protocols.3
There is a substantial amount of literature on HAI in hemodialysis units (HU) for outpatients.4,5 Most reports on this subject focus specifically on bloodstream infections (BSI) or local access infection (LAI).6,7 Also, the vast majority of studies were conducted in developed countries.4 Since benchmarking is a useful tool for measuring the effectiveness of infection control policies, data on the incidence of HAIs in hemodialysis in developing countries are needed.
In 2011, the Brazilian Society of Nephrology estimated that there were 45,000 patients undergoing hemodialysis in Brazil.8 Approximately 91% of patients’ therapies were supported by the Brazilian Public Health System (“Sistema Único de Saúde” – SUS). Though there are governmental rules for collecting HAI data in HU, no public report is presently available.9 Our study aimed to contribute to the knowledge on this issue, presenting and analyzing data on the epidemiology of HAI in a HU in the city of Botucatu, São Paulo State, southeastern Brazil.
The HU is affiliated to the Botucatu Medical School teaching hospital. It is the reference for hemodialysis for an area comprising 500,000 inhabitants. Prospective active surveillance of HAIs has been carried out since March 2010. Our study focuses on data from March 2010 through May 2012. Surveillance methods included daily visits to the unit, inspection of catheters access sites and real-time review of medical charts. We also performed monitoring of microbiological results. The HAI definitions followed the Centers for Diseases Control and Prevention (CDC) guidelines.10 The incidence density of BSI and LAI was expressed in infections per 1000 access-days. Incidence was calculated for groups using different vascular accesses: temporary catheters; permanent catheters; grafts; or arteriovenous fistulas. For all other HAIs, incidence was expressed in infections per 1000 patient-days.
Comparisons of groups were performed using the mid-p exact test in OpenEpi software (©Emory University, Atlanta, USA). Forest plot charts were built in a free online applicative (http://www.stattools.net/ForestPlot_Pgm.php).
We also assessed the temporal behavior of those infections, using Shewhart control charts.11 Briefly, we built charts based on the Poisson distribution (also known as u-charts). Monthly incidence rates were used. The mean rate (u) was calculated for the whole period with the following formula:

The standard error (sigma) was obtained for each month with the formula:

Finally, we defined “upper warning limit” (UWL) and “upper control limit” (UCL) as two and three sigma values above the mean rate, respectively. Following guidelines proposed by Sellick,11 we defined atypical occurrences based on the finding of one month's incidence above the UCL or values above UWL for two consecutive months.
During the study period, a total of 49,831 patient-days were counted, which was equal to the sum of access-days. The number of access days for specific groups was: temporary catheter, 2460; permanent catheter, 19,110; graft, 900; fistula, 27,361.
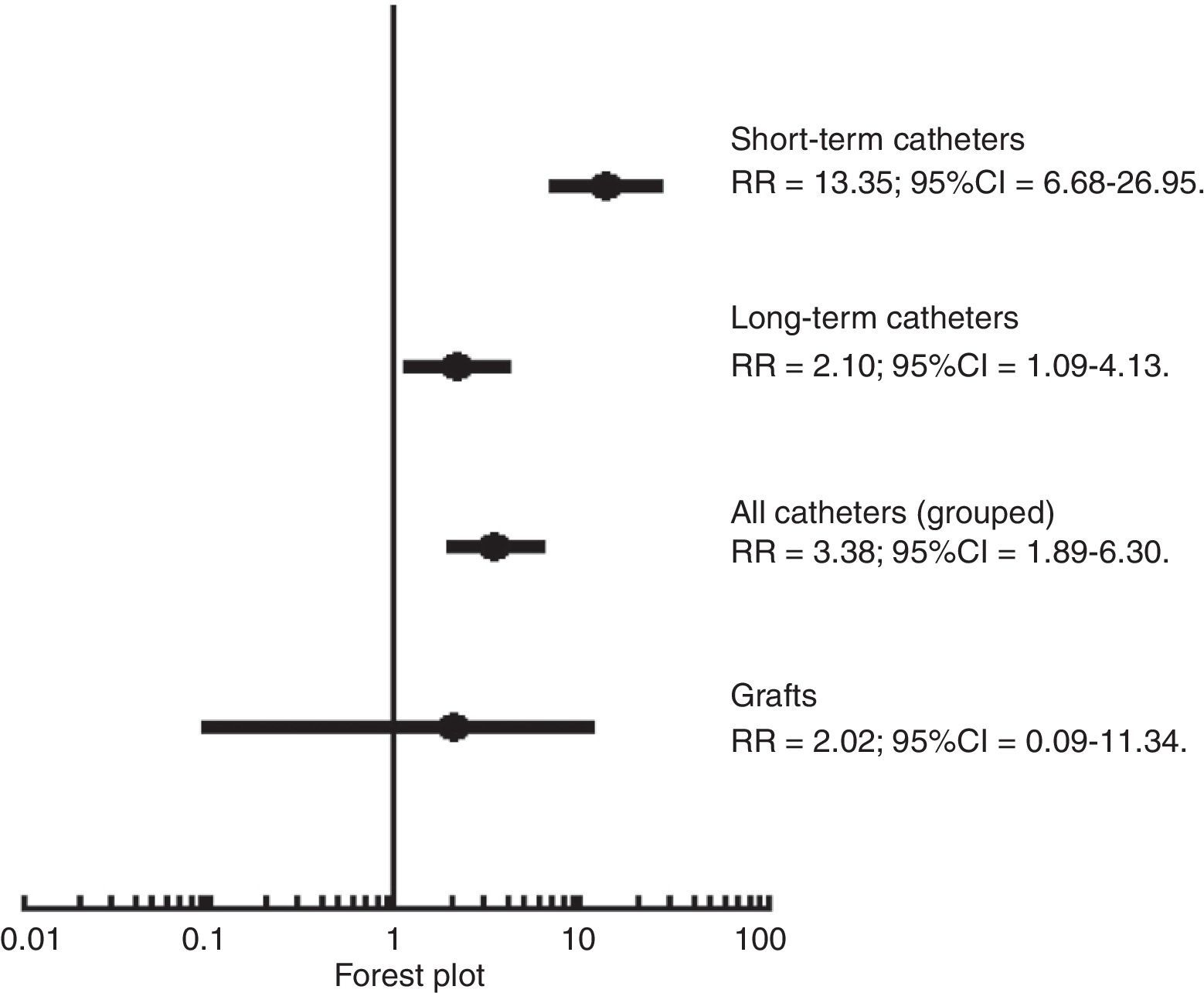
The pooled BSI incidence for the study period was 1.12 per 1000 access-days (95% confidence interval [CI], 0.86–1.45). The incidence (per 1000 access-days) for access groups was as follows: temporary catheters, 7.32 (95% CI, 4.47–11.34); permanent catheters, 1.15 (95% CI, 0.74–1.71); grafts, 1.11 (95% CI, 0.06–5.48), and fistula, 0.55 (95% CI, 0.32–0.88). The BSI incidence was significantly higher (p<0.05) for both catheters groups, as compared to the fistula group (Fig. 1). The most frequent agents of BSI (recovered from blood cultures) were: Staphylococcus aureus (36.6%), coagulase-negative staphylococci (CoNS; 20.0%), Klebsiella spp. (16.7%), and Pseudomonas aeruginosa (15.0%). Other Gram-negative bacilli accounted for 13.3% of cases. The resistance pattern of those agents was noteworthy. Among Gram-positive cocci, resistance to methicillin was found in 72.7% of S. aureus and 100% of CoNS. Gram-negative bacilli were also often multidrug-resistant. Resistance to third generation cephalosporins was found in three out of ten Klebsiella spp. and in the two Escherichia coli strains causing BSI in the study period. On the other hand, P. aeruginosa resistance to carbapenems (11.1%) and ceftazidime (22.2%) was low.
 of the incidence of bloodstream infections related to several vascular accesses, using arteriovenous fistula as a reference category. Note. RR, rate ratio; CI, confidence interval.")
The pooled LAI incidence was 3.80 (95% CI, 3.30–4.39) per 1000 access-days. The incidence was significantly higher for patients with permanent catheters (9.58; 95% CI, 8.26–11.04) when compared to those with temporary catheters (2.03, 95%CI, 0.66–4.74). LAI incidence for fistulas was 0.07 (95% CI, 0.01–0.24) per 1000 access-days. There was no LAI in grafts in the study period.
Incidence rates for other HAI (per 1000 patients-day) were as follows: upper respiratory infections, 1.72 (95% CI, 1.35–2.16); pneumonia, 1.35 (95% CI, 0.73–1.97); urinary tract infections (UTI), 1.25 (95% CI, 0.94–1.93); skin/soft tissues infections, 0.93 (95% CI, 0.67–1.26); other sites, 0.12 (95% CI, 0.04–0.27). Gram-negative predominated among agents of UTI: Klebsiella spp. (33.9%), E. coli (27.5%), Enterobacter (14.5%) and P. aeruginosa (14.5%). Two thirds of Klebsiella and E. coli isolates produced extended-spectrum beta-lactamases.
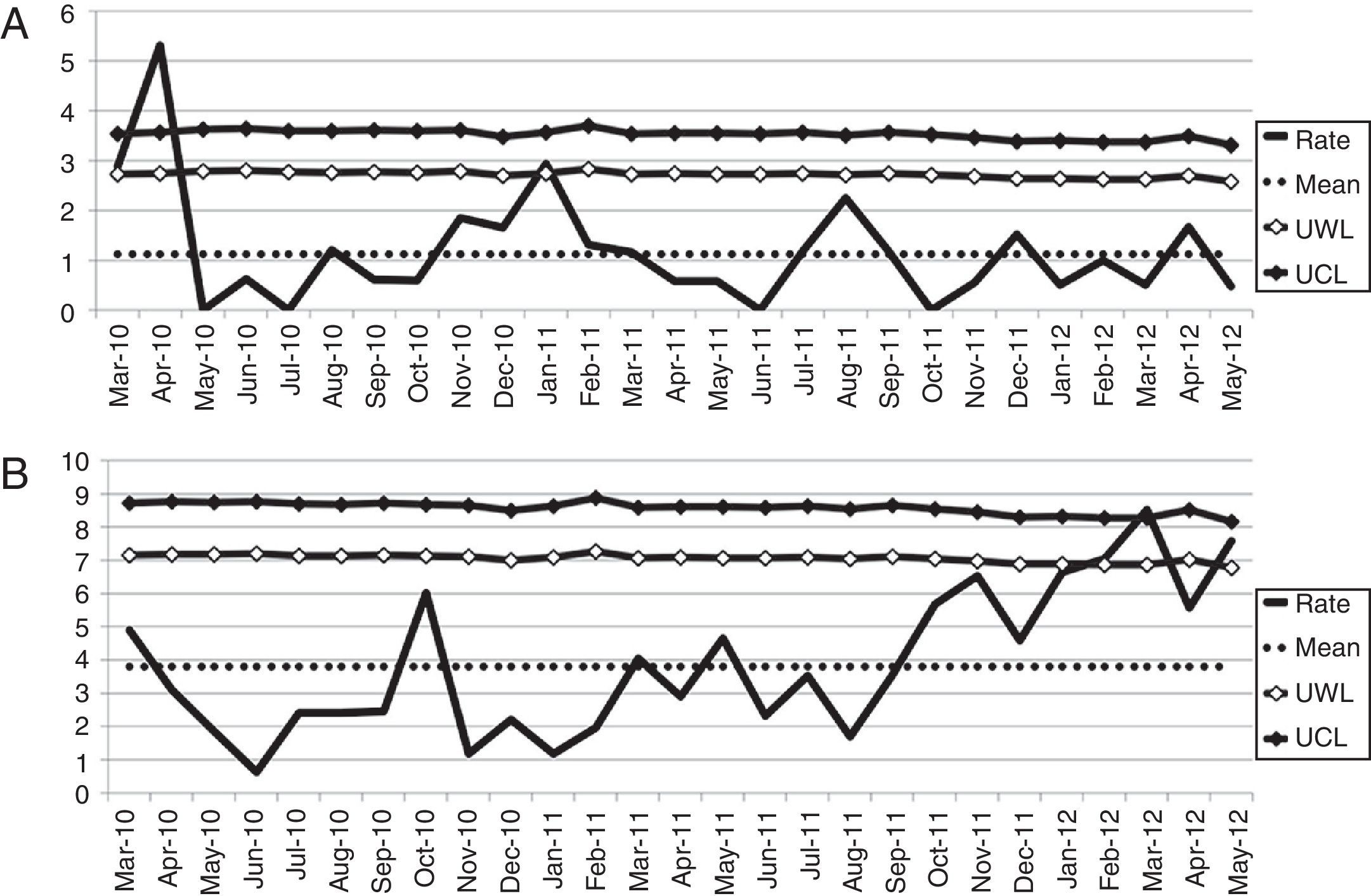
We used control charts to analyze temporal behavior of BSI and LAI (Fig. 2). The charts characterized an outbreak of BSI caused by P. aeruginosa, on April 2010, comprising seven cases, which on investigation proved to be related to contamination of water supply. We also detected a rise in the incidence of LAI in the end of the study period, concurrently with the hiring of new nursing personnel.
 and local access infections (B). Note. UWL, upper warning limit; UCL, upper control limit.")
There are similarities between infections occurring in hospital wards and those affecting outpatients on hemodialysis. This is particularly true for catheter related infections. In fact, both BSI and LAI are similar to their nosocomial counterparts in terms of etiology, pathogenesis, and prevention.12 It is somewhat surprising that epidemiological tools from nosocomial infection surveillance are rarely applied in HU.
Benchmarking is one of those valuables tools for infection control.13 The comparison of particular units with aggregate data from multicenter surveillance provides a basis for self-assessment and for establishing policies and goals. The most complete data for benchmarking of hemodialysis-related infections were reported by the CDC's National Healthcare Safety Network (NHSN).13 NHSN data was expressed in infections per 100 patient-months. When we converted our data to that unit, BSI incidence values were as follows: 3.5 (permanent catheter), 21.9 (temporary catheter), 3.3 (graft) and 1.7 (fistula). The NHSN data for these groups are 4.2, 27.1, 0.9 and 0.5, respectively. Even though the incidence of catheter-related BSI in our institution was slightly lower than that reported by NSHN, it was three times higher for patients using grafts and fistula. On the other hand, our data on LAI related to NSHN incidence in the following proportions: temporary catheters, 28.8 (our HU)/5.1 (NHSN); permanent catheters, 6.9/1.7; graft, 0/0.4; fistula, 0.2/0.2. Unfortunately, no standards for benchmarking are available for HU in Brazil.
Control charts are other important tools for HAI surveillance.11 The follow-up of monthly rates allows infection control practitioners to assess tendencies and to identify atypical situations (such as outbreaks). Control charts were particularly helpful for infection control diagnosis and policy planning in our HU in the study period. The finding of atypical incidences for BSI and LAI supported a revision of the water supply and a strategy for continuous education for nurses and nursing technicians.
Although there are few reports on infection sites other than BSI and LAI, they are by no means negligible. Recent studies have indicated hemodialysis units as sources of healthcare-associated pneumonia.14,15 Kawasaki et al. found that hemodialysis-associated pneumonia (HDAP) differed from cases arising in the community in both etiology (with predominance of Staphylococcus aureus) and severity (with high case-fatality ratio).16 The rate of HDAP in our study (1.35 per 1000 patients-day) was similar to that reported for nosocomial pneumonia among adult patients not submitted to mechanical ventilation in a Brazilian hospital (which was 1.02 per 1000 patients-day).17 This suggests that the underlying disease and exposure to healthcare do not differ between dialysis units and noncritical hospital wards. Even though further studies focusing this issue are necessary, the extension of surveillance for HDAP and other infection sites (not related to vascular devices) may be useful for timely detection and appropriate management of individual cases or outbreaks.
In conclusion, our study found that BSI and LAI and endemic in our HU, with atypical peaks related to working processes. Also, it allowed us to identify high incidence of infections in other sites, especially HDAP. Above all, our data underscore the usefulness of applying methods commonly used in hospital-based surveillance to assess the safety of healthcare for patients undergoing hemodialysis.
Conflicts of interestThe authors declare no conflicts of interest.
